Listen To Your Heart: A Patient Perspective on Catheter Ablation
– 5 min read

Undergoing a heart procedure can be a nerve-wracking experience, especially when it involves a catheter ablation. This is a first-hand account of a patient's personal journey in hospital, shedding light on the daunting procedure of catheter ablation and the promising results it should produce for patients. By Micah Gerstner
Content Warning: This article describes the personal experiences of undergoing a heart surgery in hospital, which may be distressing to some readers.
At thirteen, I first remember describing my racing heart to my parents. I had played in a basketball game earlier in the day, and I had trouble breathing, my chest hurt, and my heart was going really fast as if I was still running. At the doctor’s office, no symptoms were showing and I was misdiagnosed with asthma and dehydration. This didn’t feel right to me, but as a child I didn’t have the words to explain my symptoms as they kept happening. Seven years later, I would be hospitalised for having a heart rate of 200 bpm for 12 hours.
Supraventricular Tachycardia. SVT. A high heart rate, which can appear and stop suddenly. Patients may present with chest pain, difficulties breathing, light-headedness, anxiety, and fainting (Patti and Ashurst, 2024). When an episode lasts for a long time, you are supposed to go to the hospital to break your heart out of the rhythm. Usually I could break out of the rhythms with sleep, but when that didn’t happen, the hospital treated me with injections of adenosine flushed through my heart with saline. These treatments have the side effect of “impending doom” where you believe you will die.
Upon the recommendation of my doctors, I was advised to undergo a catheter ablation, which would involve entering my heart to find the cause of my SVT and using radiofrequency to scar over the region causing trouble. An incision in my groin will allow catheters to map the electric currents of my heart and emit the necessary frequencies. All the while, nurses will be measuring my oxygen levels, heart rate, and the output of my electrocardiogram (ECG).
In December, it was finally time to begin the procedure. At the hospital, I walked with the nurse to the electrophysiology (EP) lab. I lay down on the thin table, settling my legs into a small divider which would keep them stationary throughout the procedure. A technician placed the twelve ECG leads on my chest, side, and wrist while another shaved the area near my groin to prepare to insert the catheters. The anaesthetist connected my cannula to an IV to rehydrate me and prepare to administer any drugs. Another nurse put a blood pressure cuff and pulse oximeter on my arm and finger respectively.
Before the study began, the doctor reminded me of what was about to happen. My groin would be numbed, the catheter inserted, and the pathways of my heart explored to figure out what was causing my SVT. The team was ready. A nurse injected lidocaine into my groin to numb the region and the doctor began to lead the catheters to my vein. Even though the lidocaine numbed the pain sensation, I still felt the pressure from the catheter entering my leg. I noticed that he paused a few times while inserting the catheters, requiring him to press down again. This time I asked whether it was supposed to hurt. He called a technician to once again inject lidocaine and explained that he was struggling to get the catheter into my vein. I laughed and told the nurses that nothing is ever easy with my body.
Once he found the vein, the catheter slithered up into my torso and into my heart, entering via the inferior vena cava. He then directed the radiographer to start x-raying my heart. When I craned my head just right, I could see the live x-rays and the location of the catheters (see Fig. 1).
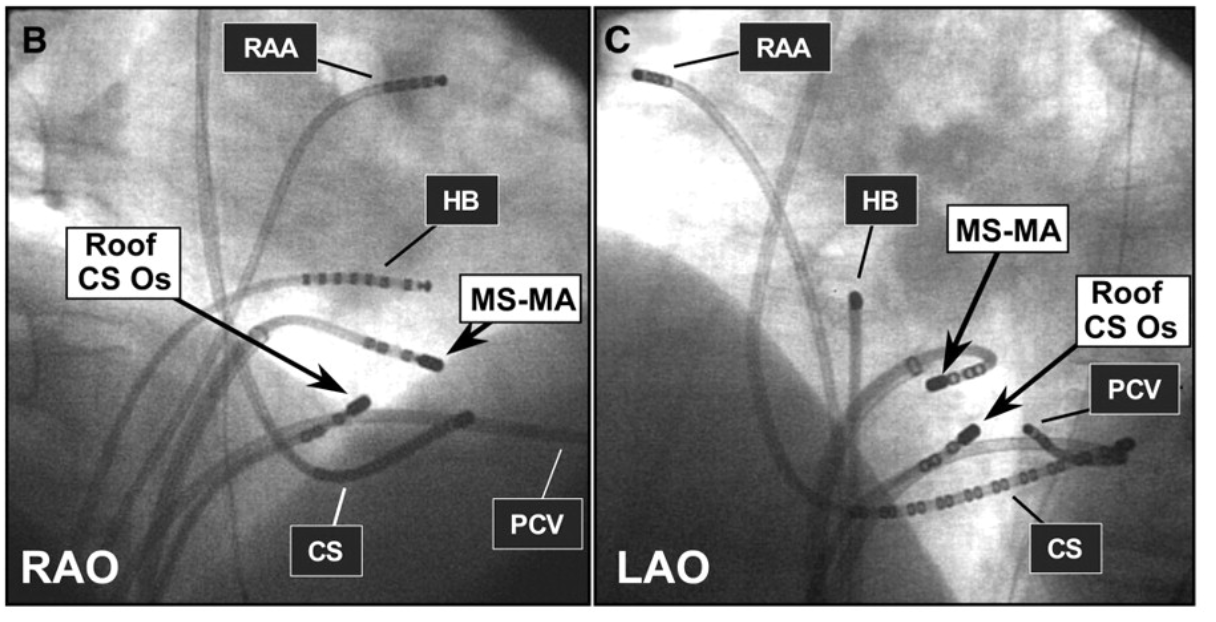
Figure 1. Two examples of x-ray imaging of the heart during catheter ablation (Nakagawa and Jackman, 2007). The catheter labelled MS-MA is an ablation catheter, which provides the energy necessary to scar the heart tissue. The other catheters are location catheters, helping map the electric currents of the heart.
One of the catheters stimulated a region of my heart, causing it to leap into action. It beat faster. Faster. The heart monitor started to blare, alerting my care team to a heightened heart rate of about 180 bpm. The doctor carefully studied the screen in front of him while the nurses reassured me that I could ignore the blaring machine. The x-ray machine whirred around me, and eventually the doctor instructed the technician to stop. At one point, he warned me that he would need to punch a tiny hole in the wall between the left and right atria, as he suspected this is where the problematic pathway is. Fifteen minutes in, he had located it. After a few moments, he told me that he is going to begin the ablation. 3… 2… 1… The catheters made a snapping sound as it zapped the troublesome pathway. My heart immediately calmed to a regular heartbeat.
They triggered the irregular heartbeat again. This process repeated for the next few hours as I lay as still as I could on the operating table. Pressure built in my leg as time continued. They decided that they must reinject the area with lidocaine. Pain built in my chest as they continued to ablate my cardiac tissue. They gave me morphine to relax. As my heart continually leapt into action and was ablated into a normal heart rate, my heels became incredibly sore as they supported my body weight. I shifted around too much and started to feel tired. Probably half an hour later, the doctor decided to end the procedure. My heart reacted too much to the ablation and the doctors are also tired.
The long catheters were pulled out of my leg, snaking their way out of my heart and back down the vena cava. Once the pulling sensation left, they removed the port and immediately placed pressure on the wound. After fifteen minutes, the bleeding stopped, and I was transported to recovery. They dripped paracetamol via IV and observed my heart rate until I was stable.
They returned me to my room, where the doctor explained that the EP study was successful. They knew what kind of SVT I have and located the area causing problems. However, the success of the ablation was in the air. We would need to wait a month before reassessment.
I spent the night in the hospital, where I had my first meal and drink in nearly 20 hours. I quickly fell into a restless sleep. In the morning, I began a few months’ course of aspirin and lansoprazole. For the next few weeks, I was told to reduce my activity and not lift anything too heavy. I felt exhausted and nearly fell asleep in the taxi back home.
Very few patients experience complications post surgery. A Singaporean cohort reported that 0.5% of patients will experience complications (Tan et al., 2022). Furthermore, 3.5% of patients will require another ablation while less than one percent will require a pacemaker up to 9 years after surgery. After the ablation, I had a typical recovery and currently show no symptoms requiring another ablation. As time continues to pass, I have become more confident and I have regained my sense of adventure knowing that my heart will be able to cooperate even if I put it under stress.
Bibliography
Cover image credit: Pexels. https://www.pexels.com/photo/surgeons-performing-surgery-in-operating-room-28782764/



